


Listen to the Audio Version
AI Summary
For more than three millennia, the resinous treasure drawn from the bark of Boswellia serrata — known throughout Ayurvedic tradition as Shallaki — has occupied a position of singular therapeutic importance in the Indian subcontinent. This article traces its extraordinary journey from the botanical descriptions of the Charaka Samhita and Sushruta Samhita through the philosophical frameworks of Tridosha theory, across the medieval consolidation of Dhanvantari scholarship, and into the crucible of modern phytochemical and clinical research. We examine how ancient knowledge systems anticipated what twenty-first-century science now confirms: that the boswellic acids concentrated within Shallaki's oleogum resin represent a uniquely potent class of anti-inflammatory agents with remarkable clinical applicability. This account is written for practitioners, historians, and educators who recognize that the authority of a botanical medicine rests not only in the laboratory, but in the living continuity of 3,000 years of observed, recorded, and transmitted healing wisdom.
Roots of a Healing Tradition: The Sacred Resin
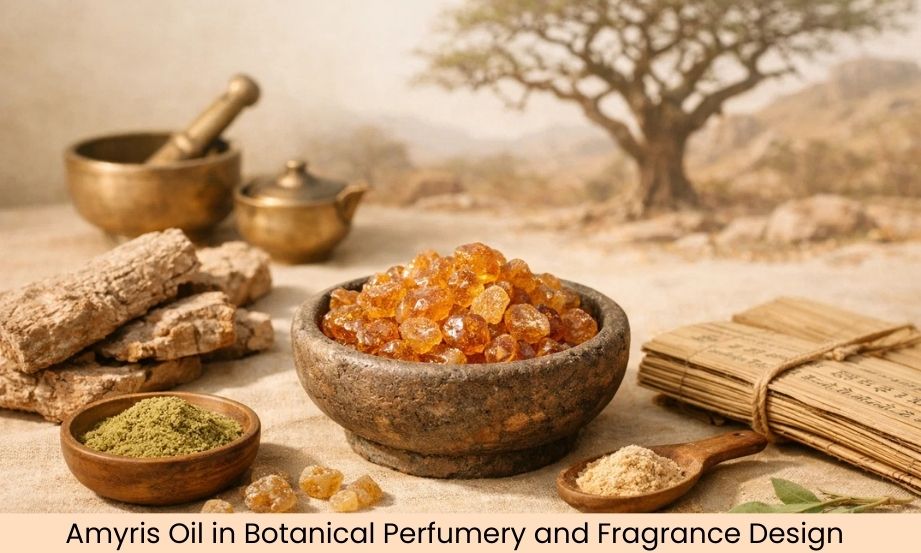
In the high, dry forests of the Deccan Plateau, the Aravallis, and the Vindhya ranges, a gnarled and resilient tree clings to rocky escarpments where few other species choose to grow. Boswellia serrata — the Indian frankincense — produces its most valuable gift under conditions of stress: when its bark is deliberately incised, the tree exudes a pale, fragrant oleogum resin that hardens into amber-colored tears. It is this resin, and the complex chemistry it conceals, that ancient Ayurvedic physicians first recognized as medicine and that modern researchers now investigate with increasing urgency.
The ecological intelligence embedded in traditional Ayurvedic botanical knowledge is immediately apparent in descriptions of Shallaki. Ancient physicians did not merely record the plant's therapeutic actions — they observed the tree's entire biography: its preferred habitat on rocky hillsides (suggesting an affinity for drainage and mineral-rich soils), its deciduous habit, the texture and color of its exudate at different seasons, and the ways in which resin collected in winter months differed in consistency and potency from that harvested in summer. This ecological attentiveness was not incidental; it was fundamental to a system of medicine in which place, season, constitution, and preparation were inseparable from therapeutic effect.
"Shallaki is the remover of kapha, the subduer of vata, the purifier of blood — and the healer of the joints that time has made to suffer." — Classical Ayurvedic aphorism
The Sanskrit name Shallaki appears across multiple ancient texts with remarkable consistency, though the plant is also referenced as Sallaki, Gajabhaksha (food of elephants — a reference to wild herds' documented consumption of the resin), and Kundurukkam in South Indian traditions. The tree belongs to the family Burseraceae, which includes the Arabian and African frankincense trees (Boswellia sacra, Boswellia papyrifera), and its resin was traded across maritime routes with Mesopotamia, Persia, and the Arab world as early as the second millennium BCE, making Shallaki not only an Ayurvedic medicine but a substance woven into the earliest chapters of global commerce.
The Resin as Philosophical Object
To understand Shallaki's place in Ayurveda is to understand that ancient Indian medical philosophy does not separate substance from meaning. The resin's bitter-astringent rasa (taste), its ushna virya (potency, here warm or heating in some classical accounts, cooling in others — a debate that persists in the literature), and its katu vipaka (post-digestive transformation) were not merely classificatory labels but active principles that predicted how the substance would interact with the three doshas — Vata, Pitta, and Kapha — that governed physiological balance.
In the classical reckoning, Shallaki's primary therapeutic domain was the pacification of aggravated Vata dosha — the biological force governing movement, neurological signaling, and joint integrity. The characteristic signs of Vata vitiation — pain, stiffness, cracking of joints, degeneration of tissues, emaciation — correspond with striking precision to the modern clinical picture of osteoarthritis, rheumatoid arthritis, and other inflammatory joint disorders. That Shallaki was prescribed for precisely these conditions across thousands of years of practice is not coincidence; it represents an epistemology of bodily observation that, while operating within a wholly different conceptual framework from Western biomedicine, arrived at therapeutically convergent conclusions.
Read Our Article
Boswellia Serrata (Indian Frankincense): Uses and Health BenefitsThe Classical Corpus: Shallaki in the Foundational Texts
The textual history of Shallaki's medical use begins in earnest with the Charaka Samhita, generally dated to the first century CE in its compiled form but drawing on oral and written traditions that may extend to 600 BCE or earlier. Charaka, the legendary physician-sage credited with the compilation, places Shallaki in the category of Vedanasthapana — agents that arrest pain — and also within the broader group of drugs that promote tissue healing (Ropana) and cleanse wounds (Shodhana). This dual action, simultaneously analgesic and healing, anticipates the modern pharmacological understanding of boswellic acids as agents that suppress leukotriene synthesis while supporting tissue regeneration.
The Charaka Samhita: First Systematic Documentation
In the Sutrasthana of the Charaka Samhita, Shallaki resin appears in formulations addressing Amavata — a condition whose symptom complex of painful, swollen, morning-stiff joints closely aligns with rheumatoid arthritis — and in preparations for Sandhivata, the wear-related joint deterioration equivalent to osteoarthritis. Charaka's descriptions are precise: the resin should be collected from trees growing on rocky terrain at higher elevations, prepared by heating over a mild fire, and combined with specific co-medications (anupanas) including cow's ghee, sesame oil, or decoctions of other Vata-pacifying herbs such as Ashwagandha (Withania somnifera) and Bala (Sida cordifolia).
The emphasis on anupana — the vehicle through which a medicine is delivered — reflects a sophisticated understanding of bioavailability that modern pharmacology has only recently begun to appreciate scientifically. Research now demonstrates that boswellic acids, particularly the most potent form acetyl-11-keto-β-boswellic acid (AKBA), exhibit significantly enhanced absorption when co-administered with lipids. The ghee and sesame oil prescribed as anupanas in classical formulations are not arbitrary additions; they are pharmacologically rational delivery mechanisms, arrived at through millennia of empirical observation.
The Sushruta Samhita: Surgical and Wound-Healing ApplicationsAsia Pacific Market Growth
Where Charaka's text emphasizes internal medicine, the Sushruta Samhita — the great treatise on surgery attributed to the physician-sage Sushruta and compiled roughly contemporaneously with Charaka — employs Shallaki within a different but complementary therapeutic register. Sushruta's chapter on wound management (Vrana Prashamsaniya) lists Shallaki resin among the most efficacious substances for promoting granulation of tissue, resisting putrefaction, and preventing the 'blackening' of wound margins — language that translates with reasonable accuracy into the modern concepts of antimicrobial action and prevention of necrosis.
Sushruta also documents Shallaki's use in bone-healing, prescribing resin-based preparations for fractures where normal repair was delayed or complicated — a context that aligns with emerging research into Boswellia's effects on osteoblast activity and cartilage matrix synthesis. The surgical tradition's interest in Shallaki reflects a recognition that the resin's anti-inflammatory properties were systemic in character, relevant not only to chronic pain conditions but to acute tissue trauma and recovery.
"The resin of Shallaki, properly prepared, closes wounds as time closes the separation between patient and health." — Sushruta Samhita (paraphrase)
Our Other Product
Evernia PrunastriThe Ashtanga Hridayam: Medieval Systematization
By the seventh century CE, the physician Vagbhata composed the Ashtanga Hridayam — the Heart of the Eight Branches — which synthesized and rationalized the Charaka and Sushruta traditions while adding substantial original clinical material. In Vagbhata's reckoning, Shallaki achieves a more systematized pharmacological profile: it is classified as Sothahara (anti-inflammatory), Vedanasthapana (analgesic), Sandhi-balya (joint-strengthening), and Raktashodhaka (blood-purifying). The blood-purifying category is particularly significant, reflecting a classical understanding that chronic inflammatory conditions arise partly from the accumulation of toxic metabolic products in the blood (Ama) — a concept with intriguing parallels to modern understanding of systemic inflammation and metabolic endotoxemia.
Classical Ayurvedic Properties of Shallaki (Boswellia serrata)
| Ayurvedic Parameter | Description |
|---|---|
| Rasa (Taste) | Tikta (bitter), Kashaya (astringent), Madhura (sweet in some classifications) |
| Virya (Potency) | Ushna (warming) — promotes circulation and dispels cold-type obstructions |
| Vipaka (Post-digestive effect) | Katu (pungent) — supports metabolic transformation |
| Guna (Qualities) | Laghu (light), Ruksha (dry), Tikshna (penetrating) |
| Dosha Action | Primarily Vata and Kapha pacifying; neutral to mildly Pitta aggravating in excess |
| Primary Indications | Amavata, Sandhivata, Vrana (wounds), Asthi-majja vikara (bone disorders), Shvayathu (edema) |
| Classical Formulations | Shallaki Ghrita, Yogaraja Guggulu combinations, Rasnasaptaka Kwatha |
Read Our Article
Health Benefits of Frankincense Serrata in IndiaMedieval Elaborations: Trade, Tantra, and Therapeutic Expansion
The medieval period of Ayurvedic scholarship (roughly 900–1600 CE) witnessed both the deepening of Shallaki's clinical applications and the expansion of its cultural resonance. As Indian Ocean trade networks intensified, Boswellia resin moved in both directions: Indian Shallaki traveled to Arab pharmacies and Unani medicine (where it was incorporated as Kundur), while Arabian frankincense occasionally supplemented or was confused with the Indian variety in coastal trading posts. This cross-cultural pharmacological exchange shaped Shallaki's identity as a medicine with a cosmopolitan history, even as its roots remained firmly planted in the subcontinent.
Dhanvantari Nighantu and the Materia Medica Tradition
The Dhanvantari Nighantu, a medieval lexicon of medicinal substances composed between the tenth and thirteenth centuries, provides one of the most detailed classical descriptions of Shallaki in its botanical, organoleptic, and therapeutic dimensions. The text distinguishes multiple grades of resin quality based on color (white or pale yellow being superior), texture (smooth and homogeneous preferred over granular), and fragrance (a clean, balsamic aroma indicating freshness and potency). These quality parameters anticipate the concerns of modern standardization, where HPLC profiling of boswellic acid content serves an analogous quality-assurance function.
The Nighantu tradition also expanded Shallaki's therapeutic indications beyond the joint and wound-healing domain to include conditions recognizable as chronic bronchitis and asthma (Shvasa), inflammatory bowel conditions (Grahani), and certain categories of fever where secondary inflammatory processes complicated recovery. Each of these extensions has found remarkable resonance in twenty-first-century clinical research, where Boswellia extracts have demonstrated efficacy not only in arthritis but in inflammatory bowel disease, asthma, and systemic inflammatory conditions — suggesting that the medieval expansion of indications was not mere speculation but the product of sustained empirical observation.
Shallaki in Regional Traditions: From Kerala to Kashmir
As Ayurveda developed distinct regional schools — the Kerala tradition of Ashtavaidya families, the Rajasthani desert medicine tradition, the Himalayan Vaidya lineages of Uttarakhand and Kashmir — Shallaki acquired local inflections while retaining its core identity. In Kerala's Keraliya Panchakarma traditions, Shallaki oil preparations (tailas) became important components of external therapy for musculoskeletal conditions, applied through the technique of Pizhichil (therapeutic oil bathing) and Abhyanga (systematic oil massage). The principle was consistent with classical doctrine: the resin's anti-inflammatory principles, when delivered transdermally through warm oil, could penetrate the deeper tissue layers (dhatus) where Vata-type pathology was rooted.
In the northern Himalayan traditions, Shallaki's use reflected the ecological reality of communities living at altitude, where cold, dampness, and physical exertion created endemic joint complaints from early adulthood. Here, the resin was often consumed in milk decoctions (Kshira Paka) — a preparation method that again demonstrates pharmacological sophistication, since milk's fat content would enhance the bioavailability of the resin's lipophilic boswellic acid constituents.
Our Other Product
Balsam ToluThe Chemistry of Tradition: What Science Found
The story of Boswellia serrata's transition from Ayurvedic classical text to the pages of peer-reviewed pharmacology journals is itself a lesson in the productive tension between traditional knowledge and scientific method. Initial interest from European and American researchers in the mid-twentieth century was fitful and somewhat dismissive — the plant was studied primarily in the context of its relationship to Arabic frankincense, which carried more immediate cultural familiarity for Western scientists. It was the work of German researcher Heinz Schippe and subsequently a generation of Indian pharmacologists and phytochemists, particularly those working at institutions including the Central Drug Research Institute (CDRI) in Lucknow and the Indian Institute of Integrative Medicine in Jammu, that elevated Shallaki research to scientific rigor.
Boswellic Acids: The Active Architecture
The oleogum resin of Boswellia serrata comprises three primary fractions: essential oils (approximately 5–9%), resin (60–65%), and gum (25–30%). The resin fraction contains the pharmacologically most significant constituents — the pentacyclic triterpene acids collectively termed boswellic acids. At least six major boswellic acids have been characterized: β-boswellic acid, 3-O-acetyl-β-boswellic acid (ABA), 11-keto-β-boswellic acid (KBA), and the compound now considered most potent, 3-O-acetyl-11-keto-β-boswellic acid (AKBA).
AKBA's primary mechanism of action — selective inhibition of 5-lipoxygenase (5-LOX), the enzyme responsible for leukotriene synthesis — represents a pharmacological pathway categorically distinct from the NSAIDs that dominate conventional anti-inflammatory therapy. NSAIDs inhibit cyclooxygenase enzymes (COX-1 and COX-2), suppressing prostaglandin synthesis but leaving the leukotriene pathway intact and often causing gastrointestinal damage as a collateral consequence of COX-1 inhibition. AKBA's selectivity for 5-LOX offers anti-inflammatory efficacy without the gastric and renal risks associated with prolonged NSAID use — a distinction with enormous clinical significance for the management of chronic inflammatory conditions where long-term medication is required.
Additional Mechanisms: A Multitarget Medicine
Research since the 1990s has revealed that Shallaki's anti-inflammatory profile cannot be reduced to 5-LOX inhibition alone. AKBA has been shown to inhibit the pro-inflammatory transcription factor NF-κB, suppressing the upstream regulatory cascade that governs the expression of multiple inflammatory cytokines including TNF-α, IL-1β, and IL-6. Separately, boswellic acids demonstrate inhibition of human leukocyte elastase (HLE), a protease enzyme implicated in cartilage destruction in rheumatoid arthritis. These complementary mechanisms — operating at different points in the inflammatory cascade — begin to explain clinically why Shallaki's therapeutic effects in chronic conditions often exceed what would be predicted from 5-LOX inhibition alone.
Perhaps most intriguingly from a classical Ayurvedic perspective, research has documented Boswellia's effects on synovial fluid viscosity and cartilage glycosaminoglycan content — markers of structural joint health — suggesting that the classical designation of Shallaki as Sandhi-balya (joint-strengthening) captures a genuine biological reality rather than merely a metaphorical aspiration.
"The ancient physicians described the action. The modern laboratory has found the mechanism. Neither is complete without the other."
| Compound | Description |
|---|---|
| AKBA (3-O-acetyl-11-keto-β-boswellic acid) | Most potent 5-LOX inhibitor; primary anti-inflammatory agent |
| KBA (11-keto-β-boswellic acid) | Significant anti-inflammatory activity; synergistic with AKBA |
| ABA (3-O-acetyl-β-boswellic acid) | Contributes to NF-κB inhibitory activity |
| β-Boswellic acid | Backbone structure; less potent but present in highest concentration |
| Essential Oils (α-thujene, p-cymene, limonene) | Contribute to antimicrobial and aromatherapeutic properties |
| Gum fraction | Polysaccharide components with potential immunomodulatory activity |
Clinical Evidence: 3,000 Years Subjected to Trial
The weight of modern clinical evidence supporting Shallaki's therapeutic efficacy would, by any reasonable measure, satisfy a regulatory authority's requirements for a category of 'well-established medicinal use' — a standard applied in European traditional medicine frameworks. More than forty randomized controlled trials have evaluated Boswellia serrata extracts across a range of inflammatory conditions, with the preponderance of high-quality studies focusing on osteoarthritis of the knee, inflammatory bowel disease (specifically Crohn's disease and ulcerative colitis), and bronchial asthma.
Osteoarthritis: The Joint that Memory Built
A landmark systematic review and meta-analysis published in PLOS ONE (2014) analyzed the evidence from multiple randomized controlled trials of Boswellia serrata extract for knee osteoarthritis and concluded that the evidence for significant reduction in pain and improvement in physical function was robust, with effect sizes comparable to conventional NSAIDs but without the adverse event profile associated with long-term NSAID use. The most studied commercial preparation, a standardized extract enriched to contain a defined AKBA percentage (commonly branded as 5-Loxin or Aflapin in research literature), demonstrated clinically meaningful improvements in WOMAC pain and stiffness scores within 90 days of treatment at doses of 100–250 mg daily.
What the clinical literature describes in statistical terms — reduction in joint pain scores, improvement in walking distance, decrease in morning stiffness — translates, in the lives of patients, into the restoration of mobility that classical texts described as the essence of Vata-related suffering. The physician who prescribed Shallaki in ancient Kashi and the rheumatologist who recommends a standardized extract in contemporary Mumbai are, in a very real sense, participating in a continuous therapeutic tradition.
Inflammatory Bowel Disease: An Unexpected Extension
Perhaps the most striking modern clinical application of Shallaki — and one that the classical texts did not fully anticipate in its mechanistic specificity — is its efficacy in inflammatory bowel disease. Multiple clinical trials have demonstrated that Boswellia serrata extracts are comparable in efficacy to sulfasalazine (the standard pharmaceutical treatment for ulcerative colitis) for inducing and maintaining remission, with a substantially more favorable adverse effect profile. The mechanism appears to involve inhibition of both 5-LOX and NF-κB pathways in intestinal mucosal cells, reducing the cascade of inflammatory mediators that perpetuates the mucosal damage characteristic of IBD.
From a classical Ayurvedic perspective, this application maps onto the category of Grahani — a complex of digestive and intestinal disorders that Ayurvedic texts associated with impaired Agni (digestive fire) and the accumulation of Ama (metabolic toxins) in the intestinal channels. The modern scientific understanding of IBD as a disorder of mucosal immune dysregulation and the classical Ayurvedic understanding of Grahani as a disorder of digestive intelligence are, at their therapeutic intersection, resolved by the same plant.
Asthma and Respiratory Inflammation
A double-blind, placebo-controlled trial published in the European Journal of Medical Research demonstrated that Boswellia serrata extract administered three times daily for six weeks produced significant improvement in asthma symptoms, respiratory function (forced expiratory volume and peak expiratory flow rate), and reduction in circulating eosinophil counts in 70% of treated patients — compared to 27% in the placebo group. The 5-LOX inhibitory mechanism is directly relevant here: leukotrienes, particularly leukotriene C4 and D4, are primary mediators of bronchospasm, and their inhibition by AKBA reduces the bronchoconstrictive tendency that defines asthmatic pathology.
Again, the classical correspondence is illuminating. Ayurvedic texts describe Shallaki's indication in Shvasa (respiratory distress, including conditions resembling asthma) as mediated through its ability to clear obstructed respiratory channels (Pranavaha Srota) and reduce the excess Kapha that, in the classical model, occludes airway flow. The leukotriene-mediated bronchospasm of modern pathophysiology is, from a different epistemic vantage, the Kapha-and-Vata obstruction of classical pneumatology — different frameworks describing a biological reality that Shallaki addresses in both.
Ecological Crisis and the Sustainability Imperative
No account of Shallaki's historical and contemporary significance would be complete without acknowledging the ecological crisis that now threatens the very populations of Boswellia serrata that sustained three millennia of traditional use. A 2019 report in Nature Sustainability by Gebrehiwot et al., focusing on Boswellia species across Africa and India, documented a pattern of population fragmentation, reduced regeneration, and aging tree demographics that portend significant decline in wild Boswellia populations within the coming decades without substantial intervention.
In India, the pressures are multiple and interacting: destructive tapping practices that over-harvest resin from individual trees (reducing resin yield in subsequent seasons and weakening tree immunity to pathogens), conversion of forest habitat to agriculture, overgrazing that prevents seedling establishment, and fire regimes altered by human activity. The explosion of global demand for Boswellia products — driven by the same scientific validation of efficacy that this article celebrates — has placed extraction pressure on wild populations that were never designed to supply a global nutraceutical market.
Classical Ethics and Contemporary Responsibility
Ayurvedic tradition anticipated this tension. The classical texts contain explicit guidance on ethical harvesting — proscriptions against stripping bark from the trunk during the hot season, requirements to leave adequate cambium undamaged to ensure tree recovery, and injunctions against harvesting more than a tree could sustain. These guidelines were not merely pragmatic conservation advice; they reflected a cosmological orientation in which the physician's relationship to medicinal plants was reciprocal and obligatory, grounded in the concept of Ahimsa (non-harm) extended to the natural world.
Contemporary Ayurvedic practitioners and botanical supplement companies who wish to work with Shallaki in integrity are called to honor this classical ethical framework through concrete supply-chain commitments: sourcing from certified sustainable wildcrafting operations, supporting cultivation programs that reduce pressure on wild populations, partnering with organizations working on Boswellia forest regeneration, and communicating transparently with consumers about the ecological realities of this precious resin.
"To heal with Shallaki while destroying the trees that produce it would be to violate the very principle of Ahimsa that Ayurveda places at the foundation of all medicine."
Formulation, Standardization, and the Modern Practitioner
For the Ayurvedic practitioner, herbalist, or integrative medicine clinician navigating the contemporary landscape of Boswellia products, the question of formulation and standardization is both pharmacologically significant and epistemologically complex. The classical texts prescribed the whole resin — complete with its full complement of boswellic acids, essential oils, gum polysaccharides, and minor constituents — in preparations ranging from simple powders (churnas) and resin pills (gutikas) to complex multi-herb formulations and medicated oils. Modern commercial products range from minimally processed resin powders to highly concentrated extracts standardized to defined AKBA percentages, and the evidence base for efficacy is substantially stronger for the latter category.
The Standardization Debate
The tension between whole-resin preparations and standardized extracts is, in essence, a specific instance of the broader debate in phytomedicine between full-spectrum botanical preparations and isolated or concentrated bioactive fractions. Classical Ayurvedic philosophy unambiguously favors the whole plant preparation on grounds of synergy (the principle that multiple constituents acting in concert produce effects not predictable from individual components) and safety (the argument that the full plant matrix moderates the activity of any single constituent).
Modern pharmacological research provides some support for both positions. Head-to-head comparisons of whole resin preparations and AKBA-standardized extracts in clinical trials generally show superior efficacy for standardized preparations in terms of dose-efficiency and reproducibility — but also raise the concern that some of the gastric intolerance occasionally reported with high-dose AKBA preparations may be moderated by the presence of other resin constituents in whole preparations. The clinically pragmatic answer, for most applications, appears to be standardized extracts providing a defined AKBA content within a matrix that preserves some of the whole-resin complexity — precisely the approach taken by the most rigorously studied commercial preparations.
Dosing, Safety, and Drug Interactions
The classical texts recommend Shallaki doses in the range of 3–10 grams of crude resin daily, consumed with appropriate anupana. Modern standardized extract preparations are typically dosed at 300–500 mg two to three times daily (delivering an AKBA content of 10–30% of the extract weight). Shallaki's clinical safety profile is consistently reported as favorable across clinical trials, with the most commonly noted adverse events being mild gastrointestinal discomfort at higher doses — manageable by administration with meals and lipid-containing foods, consistent with classical anupana recommendations.
Clinically relevant drug interactions are a consideration: Boswellia's inhibition of cytochrome P450 enzymes (particularly CYP3A4 and CYP2C9) has been documented in vitro and should be considered when Shallaki is used alongside medications metabolized by these pathways, including certain statins, calcium channel blockers, and immunosuppressants. This is an area where the classical texts, operating in a pre-pharmaceutical era, offer limited guidance, and where the contemporary practitioner's pharmacological literacy becomes essential.
Shallaki in the Living Tradition: Pedagogical and Philosophical Dimensions
For Ayurveda educators, the story of Shallaki offers an exemplary case study in the epistemological continuity between classical knowledge and modern science — and, equally importantly, in the places where the two frameworks diverge in illuminating ways. The medicinal efficacy of Shallaki is, by any reasonable scientific standard, established. But to teach Shallaki only as a source of AKBA, a 5-LOX inhibitor, a molecule with a particular IC50 value for leukotriene synthesis suppression, is to produce practitioners who may dispense effective medication while remaining blind to the richer understanding that classical training offers.
Teaching the Whole Story
A complete Ayurvedic education in Shallaki should encompass: the tree's ecology and the relationship between its habitat and its medicinal potency; the classical rasa-virya-vipaka analysis and its implications for constitutional prescribing; the historical trajectory from Vedic herb lore through Charaka and Sushruta to medieval Nighantu codification; the pharmacological validation of classical indications; the ethical dimensions of sustainable sourcing; and the practical clinical questions of formulation, dosing, and safety monitoring.
This integrated teaching approach models the epistemological pluralism that defines Ayurveda at its best — a system that holds empirical observation, philosophical framework, textual authority, and clinical pragmatism in productive tension rather than sacrificing any one to the others. Shallaki teaches this lesson with particular clarity because its three-thousand-year clinical record is rich enough to sustain analysis from all these perspectives simultaneously.
The Question of Knowledge Validation
Implicit in the story of Shallaki is a methodological question that practitioners and educators should engage explicitly: what does it mean for traditional Ayurvedic knowledge to be 'validated' by modern science? The most common interpretation — that a traditional medicine is 'validated' when randomized controlled trials confirm efficacy — is simultaneously practically important and epistemologically limited. It is important because it provides a shared language with evidence-based medicine and supports integration of Ayurvedic practice into pluralistic healthcare systems. It is limited because it collapses three thousand years of sophisticated, reflexive clinical observation into a single criterion — the double-blind RCT — that is neither the only legitimate form of clinical knowledge nor one that adequately captures the complexity of Ayurvedic constitutional prescribing.
The validation that Shallaki's story actually demonstrates is bidirectional: modern science confirms what classical observation established, but classical observation also contextualizes and enriches what modern science can show. The classical insistence on anupana, for example, is not merely a cultural practice that modern science has incidentally confirmed to be bioavailability-enhancing; it is evidence that a different epistemological system, operating through different methods over a far longer timeframe, arrived at pharmacological insights that the reductionist methods of twentieth-century pharmacognosy could only detect after it had developed the appropriate tools.
"The validation of Ayurveda by science is a conversation, not a verdict. Shallaki has been speaking for three thousand years."
Conclusion: The Living Tree and the Long Tradition
The Boswellia serrata tree, clinging to its rocky hillside above the Deccan plateau, is indifferent to the debates that its resin has generated across three millennia of medical history. It produces what it has always produced: a pale, fragrant exudate that contains, as if by the economy of nature, precisely the chemical architecture needed to interrupt the inflammation cascade that erodes human joints, disrupts human intestines, and constricts human airways. Whether this chemistry is described in the language of Vata pacification and Ama elimination, or in the language of 5-LOX inhibition and NF-κB suppression, the tree's gift to human health remains the same.
What changes across three thousand years is not the medicine but the frameworks through which humans have understood it, transmitted it, and applied it. The physician-sages who composed the Charaka and Sushruta Samhitas, the medieval Vaidyas who expanded and systematized their inheritance, the twentieth-century pharmacologists who subjected that inheritance to reductive analysis, and the twenty-first-century integrative clinicians who now seek to hold both the classical and scientific frameworks in productive dialogue — all are participants in a single extended conversation about how this particular resin heals, and why it matters.
The authority that Shallaki carries in contemporary Ayurvedic and integrative medical practice rests on all of these layers simultaneously. It is a medicine whose efficacy has been observed across more human lifetimes than any clinical trial could encompass, whose mechanisms have been elucidated at the molecular level with increasing precision, and whose story is inseparable from the ecological, philosophical, and ethical traditions that gave it meaning before science gave it mechanism.
For practitioners, historians, and educators who work at the intersection of traditional and modern medicine, Shallaki offers both a model and a call. The model is one of rigorous, patient, cross-generational knowledge-building that neither dismisses empirical tradition nor defers uncritically to it. The call is to carry this medicine forward with the same integrity that sustained it across three millennia — honoring the trees that produce it, the traditions that preserved it, the science that illuminated it, and the patients whose relief it continues to offer.
Recent Posts
- Floral Green Fragrance Bases: Formulating With Narcissus Absolute Alternatives in Modern Perfumery
- Indian Oud Reconstitution vs. Natural Oud: Cost Effectiveness, Performance, and Quality Comparison for Bulk Buyers
- Reconstituted Oud Blending Guide: Dihydroambrettolide, Benzyl Acetone, and Ester Based Components for Professional Fragrance Formulation
- Geranium Oil Varieties Egyptian Reunion and Madagascar Geranium Compared
- Frankincense Serrata in Premium Incense Manufacturing
- Balsam Tolu vs Balsam Peru
- Vetiver Oil in Fresh Green and Woody Fragrances
Copyright @ 2026 | BMV Fragrances Private Limited | All Rights Reserved
Website Design & Digital Marketing by webmasterindia.
Website Updated On: